COVID shot shedding? Officials say impossible (because shots aren't gene therapy)

In part one of this article, a new research study was presented which strongly suggests that simply being in the proximity of people who have been injected with the COVID shots can have serious consequences. Mainstream medicine and its institutions by and large deny that this “shedding,” as it is called, is possible with the COVID shots — although ruling it out makes various unusual findings very hard to explain.
CDC: No such thing as shedding
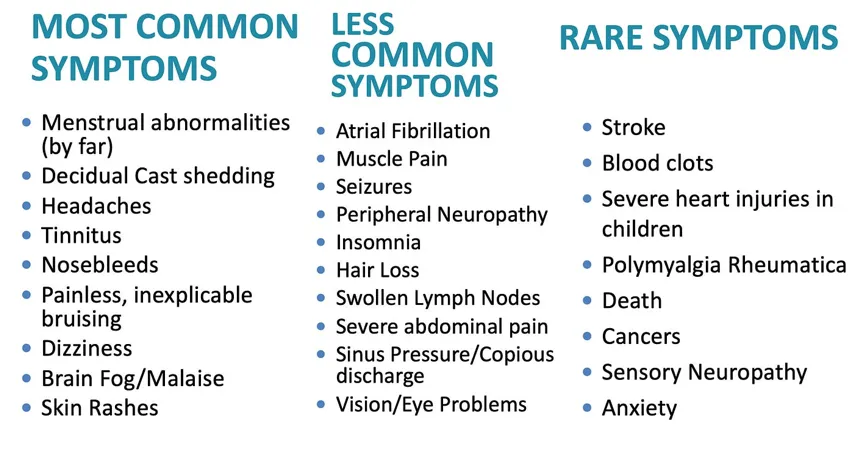
The research article investigating shedding focused on menstrual problems for the simple reason that they have been found to be the most usual problems to occur as a result of secondary exposure to the shots (aka shedding). However, contact with an injected person can have many effects on a sensitive person, as thousands of personal accounts reveal, which are summarized in this graphic:
Nonetheless, the CDC persists in its denial that shedding is a possibility with the COVID shots. It does admit that shedding is a known phenomenon with vaccines — it just claims that it’s impossible with the COVID shots because they don’t contain live virus:

Pfizer: We'll call it 'exposure' and check for that
The CDC's protestations aside, Pfizer did take the possibility of shedding into account as they launched clinical trials into their new mRNA substance. The clinical trial documents instruct investigators to report various kinds of “environmental exposures,” in which a person participating in the trial came into close contact with a non-participator — even after the trial had concluded.
These exposures include not only intimate contact but also “inhalation or skin contact” with the substance being tested i.e., the shots, for example (from Pfizer’s documents):
... a female family member or healthcare provider who reports that she is breastfeeding after having been exposed to the study intervention by inhalation or skin contact.
Pfizer even considered the possibility that something (what, precisely, is not specified) might transfer from a male exposed to the shot substance via inhalation or skin contact, to a female partner, and that this could then be transferred onward to a baby conceived at approximately the same time. This is referred to as “secondary shedding.”
A male family member or healthcare provider who has been exposed to the study intervention by inhalation or skin contact then exposes his female partner prior to or around the time of conception.
It stays in the shoulder — how could it shed?
The general public was not made aware of these concerns. What people were told was that the substance injected remained in the shoulder muscle where it swiftly degraded (after doing whatever it was supposed to do). These claims appeared on official websites from the start of the shots’ rollout, before disappearing in 2022.
It was known long before then, however, that the mRNA substance certainly did not remain in the shoulder but distributed itself widely around the body. Several studies showed that the spike protein itself wound up in every single organ in the body; autopsies found spike protein in the heart, the brain, muscles, and the vascular system.
Furthermore, animal bio-distribution studies showed that it continued to circulate for at least a month — and, that it could be detected in breast milk, i.e., shedding.
And then it shows up in mother's milk...
In August, 2021, Nature published a study confirming shedding (without using the term) in mother’s milk — this time, in human mothers. Out of 40 women studied, “vaccine” mRNA was found in the milk of 4 of them, a 10-percent shedding rate. Other studies followed confirming these findings. A study in the Lancet stated the facts bluntly:
Our findings demonstrate that the COVID-19 vaccine mRNA is not confined to the injection site but spreads systemically and is packaged into breast milk extracellular vesicles.
Furthermore, a confidential report by Pfizer showed that its researchers were aware that the mRNA (or whatever substance was being shed) in mother’s milk could harm babies who ingested it (as several studies later confirmed). 215 nursing mothers reported exposure to the mRNA (most appear to have been injected although this is not made entirely clear). 43 babies experienced an adverse event of a “non-severe” kind while 10 had a serious adverse event (such as swelling of lymph nodes, peeling skin, swollen skin).
All drug producers are required to conduct not only clinical trials but also post-marketing (PM) studies. Pfizer is no exception. Following a Freedom of Information Act (FOIA) request, the European Union released one of its periodic safety reports based on post-marketing surveillance. It contains documentation of nursing babies who experienced strokes, convulsions, and respiratory failure in association with exposure to mRNA via their mothers who received the shots.


The EU concluded that these cases were not related to the fact that the babies’ mothers got the shots, because they were “only” exposed to mRNA in the milk they drank.
Other cases of serious adverse events were similarly dismissed because they “involved exposures to the vaccine during the mother’s pregnancy.”
And then it finds its way across the placenta...
What of pregnancy? Doesn’t the placenta protect the growing fetus from dangerous substances circulating in the mother’s body? The answer is: Not always.
Referring again to the EU report, there were 458 cases of mothers exposed to mRNA while pregnant. 248 of these cases (54 percent) involved an adverse event and 53 of them involved the death of the fetus.
Pfizer, in its own report of these events, removed 14 of these cases from consideration because the pregnant mothers had a “relevant history of endometriosis, abortion spontaneous, polycystic ovaries, [or] menstruation irregular.” The other cases are listed without comment.
Pfizer also noted that, in some cases, the mother was exposed to the mRNA via the father and did not herself receive the shot. There were two such instances described as “miscarriage of the partner.”
Studies have confirmed the presence of COVID shot mRNA in the umbilical cord and placenta of pregnant women. This shouldn’t have surprised anyone. It’s been known for years that nanoparticles (the “containers” in which the mRNA is shipped) can pass through the placental barrier (see for instance this study from 2017).
And then it flies through the air...
Not only can nanoparticles travel through the blood, they can also be exhaled and inhaled, eaten and excreted, expelled via perspiration and absorbed through the skin. There is no dispute on this. Nanoparticles have been administered therapeutically many times using such ports of entry and there are multiple studies to refer to.
And again, this should not have surprised anyone when the COVID shots were rolled out, as much of the research in this area dates back to long before the “pandemic.” For example, a paper from 2005 refers to inhalation of nanoparticles:
When inhaled, specific sizes of nanoparticles (LNP’s/exosomes) are efficiently deposited by diffusional mechanisms in all regions of the respiratory tract. The small size facilitates uptake into cells and transcytose across epithelial and endothelial cells into the blood and lymph circulation to reach potentially sensitive target sites such as bone marrow, lymph nodes, spleen, and heart.
Clinical trials are currently underway for new vaccines using the inhalation route for mRNA, not only SARS-CoV-2 but also influenza.
No! Antibodies can fly but COVID shots can't!
Despite this wealth of evidence, officially there is no such thing as COVID shot shedding. This is possibly what led a group of researchers from the University of Colorado to explain away the results of their 2023 study with a hypothesis that is far less plausible than transfer of nanoparticles.
This study documented people who had not received the shots but had been in close proximity to people who had (in this case, it was vaccinated parents and their unvaccinated children). The children developed an immune response to COVID spike protein.
The researchers took pains to rule out prior COVID infection in the children which might have explained their immunity (by testing them for antibody types — they lacked anti-N antibodies which would likely have been there if they had been infected). What the children did have were IgG antibodies (which are usually formed in response to vaccination). The researchers surmised that the IgG antibodies themselves had been transferred via aerosols...
The simplest interpretation of our results is that aerosol transmission of Ab can occur...
... despite the fact that the likelihood of that happening and also resulting in the immunization of the children is miniscule. While antibodies can be exhaled and inhaled, they break down very quickly in the air, and the chances of a sufficient quantity to cause immunity reaching someone else's respiratory tract intact are so low that this is considered impossible. (This is very different from concentrated quantities of antibodies being squirted up a person's nose.)
Nonetheless, the researchers did not consider any alternative explanations for their findings.
If COVID shots were [defined as] gene therapy it would be a different story
It should be noted that “shedding” as a term is not a pop-scientific way of referring to the phenomenon. The FDA has an entire document specifically on shedding, titled: “Design and Analysis of Shedding Studies for Virus or Bacteria-Based Gene Therapy and Oncolytic Products.”
In this document, the FDA defines shedding as:
The release of VGBT [viral or bacterial gene therapy] products from the patient by any or all of the following routes: feces (feces); secretions (urine, saliva, nasopharyngeal fluids, etc.); or through the skin (pustules, lesions, sores).
The FDA recommends shedding studies be conducted for all gene therapy products. It also notes that while shedding is most common immediately following the therapy, it can occur weeks later and can even surge at a later stage:
Shedding is most likely to occur in the period immediately following product administration, irrespective of replication competence of the VBGT or oncolytic product. A second peak of shedding may be noted in the days/weeks after administration of a replication competent product as a result of its multiplication/amplification in vivo.
There are already a number of gene therapy products on the market. One, Roctavian, used to treat hemophilia, is known to shed for at least six months following administration, as the FDA notes:
Following IV administration of 2.13 × 1014 vg/kg ROCTAVIAN, the highest vector DNA concentration was detected in the liver, followed by the lung, heart, lymph nodes, kidney, spleen, bone marrow, testis, and brain through 6 months post-administration.
It may, of course, shed for much longer. The subjects of this research were not monitored for shedding beyond six months.
But, of course, none of this is considered relevant as the COVID shots are not classified as gene therapy.
Ivermectin to the rescue once again
As with all the myriad side effects of the COVID shots, people’s responses tend to vary widely. Some people develop myocarditis; most do not. Some die suddenly and “inexplicably”; most do not. Some have strokes or develop auto-immune disease; most do not. There seems to have been virtually no research done on what makes some people highly sensitive to these new substances while most other people (seem to) escape unscathed.
Only a very small minority of the population appear to be sensitive enough to COVID mRNA products to be affected via shedding. And, since most shedding occurs immediately following injection, it is thought by some that keeping away from people right after they get their shots may be enough protection. Keeping away after booster shots seems to be particularly important, based on anecdotal accounts, which also suggest that children and the young and healthy shed more than the older and weaker.
Multiple patient reports (documented by Dr. Pierre Kory and “A Midwestern Doctor”) mention several effective ways of countering the impact of shedding, especially ivermectin and nattokinase:
Nattokinase has been my savior; it is so effective that sometimes I can't even feel the shedding. I also take ivermectin once a week and it’s also amazing.
It's time to ban these toxic substances
The study authors who most recently publicized the effects of shedding on women, many of whom have suffered life-changing injury, conclude:
After more than a year of censorship from the medical journals, our landmark study and manuscript has been published demonstrating significant circumstantial evidence that something is being shed from the COVID-19 vaccinated population to the unvaccinated population...
It has been a very long battle to get this article published. Our experience in this process has verified that medical censorship has been in full force during the “pandemic.” The journal editors and publishers fear the potential consequences of publishing anything that contradicts the “safe and effective” propaganda with which the public health authorities have bombarded us.
It is far beyond time for these toxic injections to be withdrawn from the market.
Disclaimer: The information contained in this article is for educational and information purposes only and is not intended as health, medical, financial, or legal advice. Always consult a physician, lawyer, or other qualified professional regarding any questions you may have about a medical condition, health objectives or legal or financial issues.


.webp)

