Cholesterol drugs 'shrouded in secrecy and riddled with huge financial conflicts of interest' - Professor Peter Gøtzsche

Story in a flash:
- Statin drugs, prescribed worldwide to individuals at risk of heart disease and/or who have high cholesterol, are a highly profitable class of drugs.
- Thousands of lawsuits have been filed against the FDA and manufacturers alleging serious adverse events.
- Clinical trial side effects data for statins have yet to be made public, even as people continue to suffer serious adverse effects.
Prophylactic medicine
If you go in for a routine check-up and have never experienced any chest pain, even during rigorous exercise, but have high cholesterol levels, are diabetic, are 40 to 75 years of age, or are determined to be at sufficient ASCVD (atherosclerotic vascular disease) risk after a clinician-patient risk discussion, you may be prescribed a cholesterol-lowering drug as a “first-line treatment for primary prevention of ASCVD.”[1],[2]
Patients prescribed these drugs thus join women who have been told to remove their breasts and ovaries to prevent a possible cancer even though they are completely symptom-free. Like vaccines and bone-density testing, these drugs, tests, and procedures form a part of a massive “disease-mongering” market for Pharma, in which “[t]he social construction of illness is being replaced by the corporate construction of disease," as Ray Moynihan, et al, explained in an article carried in the BMJ:
There's a lot of money to be made from telling healthy people they're sick. Some forms of medicalising ordinary life may now be better described as disease mongering: widening the boundaries of treatable illness in order to expand markets for those who sell and deliver treatments. Pharmaceutical companies are actively involved in sponsoring the definition of diseases and promoting them to both prescribers and consumers. The social construction of illness is being replaced by the corporate construction of disease. [3](Emphases added.)
Even for the stars
Angelina Jolie underwent a prophylactic double mastectomy based merely on a genetic test. But recent research cited by What Doctors Don't Tell You explains that having the BRCA 1 gene mutation (considered a potential breast cancer risk for which the genetic testing screened) may not have been the death sentence she believed it was and that she had other options:
. . . the Southampton researchers point out. One in 800 women carries mutated BRCA 1 or 2 genes, which cause just 5 percent of all breast cancers – and they’re not quite the death sentence that everyone thinks.
. . .but Angelina Jolie had more time than her doctors suggested. And a double mastectomy isn’t the only response: there were plenty of lifestyle changes that could have reduced her risk. But, then, her doctors never told her that.
Multi-billion dollar statin market
Symptom-free people are among the two hundred million worldwide,[5] including 47 million Americans, who have been prescribed statins.[6]
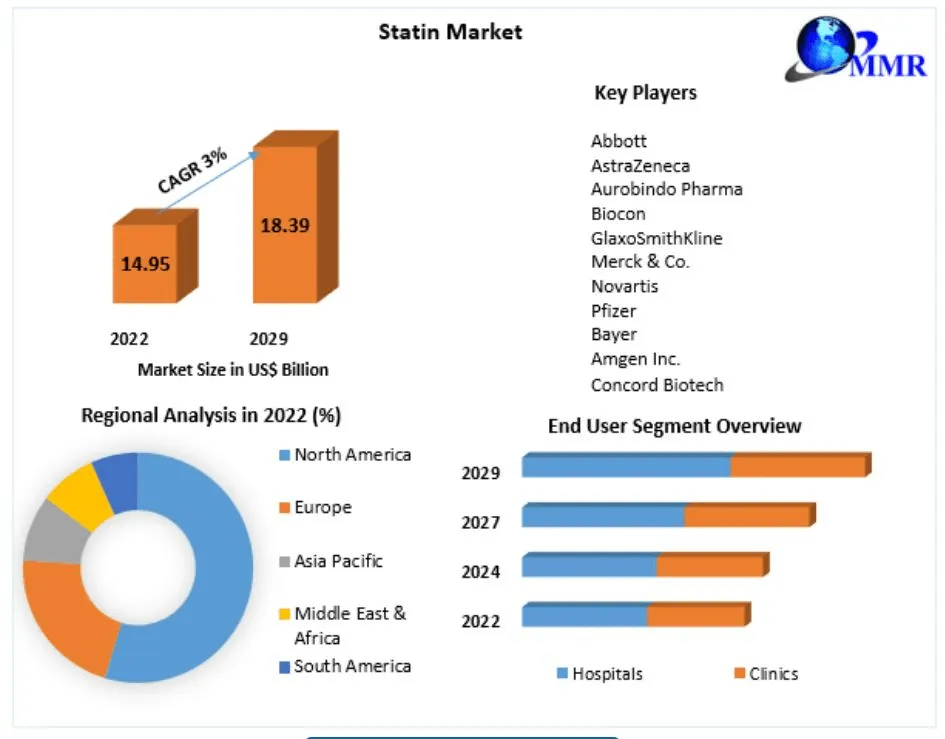
Statins, the predominant class of cholesterol-lowering drugs, are highly profitable. The worldwide statin market, according to Maximize Market Research’s graph below, is projected to grow from $14.95 billion in 2022 to $18.39 billion by 2029.[7]
Injured parties want their day in court
Asymptomatic people who are prescribed statins may assume they have nothing to lose by taking a preventive medication. However, despite their near ubiquitous use among those meeting their health department's criteria, statin manufacturers and even the FDA have been beset by statin-related lawsuits due to the serious adverse effects that thousands of statin users have experienced.[8]
Over twenty-five thousand people have filed a class action lawsuit against the FDA. They are accusing the agency of not properly evaluating the health risks associated with these drugs, as Weston reported for Law Bench. The lawsuit was filed on behalf of people who have experienced, either directly or indirectly, statin adverse effects including cardiac arrest, rashes, cognitive impairment, gastrointestinal complications, paralysis, and more:[9]
The plaintiffs in the lawsuit are asking for compensation for suffering, disability, loss of enjoyment, and funeral expenses that have resulted from these drugs. The FDA claims that it was not negligent in approving statin A. The courts, however, are considering different factors when deciding whether or not the FDA was at fault.
One factor is how the FDA approved the drug. The manufacturer of statin A had a contract with the Food and Drug Administration that dictating [sic] exactly how the drug would be approved. Other factors considered by the courts include the fact that the manufacturer knew of the risks of heart problems even before the FDA approved it and still went ahead with the release of the drug.
Pfizer has had at least two thousand lawsuits filed against it by plaintiffs claiming that the drug caused their diabetes. They have stated that the company failed to sufficiently warn patients of the drug's risks while aggressively promoting Pfizer's product over others, as USA Legal reported. Only those who took the drug before 2012, when Pfizer issued a warning, were able to join the class action suit.[10]
Nolo reporter Charles Craine, in a report on statin lawsuits, noted that Pfizer has also faced lawsuits claiming neuropathy and muscle tissue damage.[11]
Craine also noted that Bayer has been sued by thousands of people who used its statin Baycol and claimed that it caused muscle tissue damage and was linked to 31 deaths. The drug was taken off the market in 2001 and in 2005 the company paid out $1 billion to settle the lawsuits.[12]
Astra Zeneca settled a variety of lawsuits against the company for its cholesterol-lowering drug Crestor, as Drugwatch’s Elaine Silvestrini reported. [13] Those lawsuits have all been dismissed, withdrawn, or quietly settled. AstraZeneca agreed to pay $110 million to resolve a Texas whistleblower lawsuit about false and misleading marketing of Crestor and another drug under a settlement announced in August 2018. Suits for product liability include claims that Crestor caused diabetes, liver damage, and rhabdomyolysis, a serious muscle injury that can damage the kidneys.
Lawsuits said AstraZeneca failed to warn the public about the risks of taking Crestor. They also accused the company of deceptively and misleadingly promoting the drug. And they alleged AstraZeneca failed to adequately test Crestor.
Cognitive decline
Spacedoc is a website founded by a former astronaut, the late Dr. Duane Graveline, where he recorded his devastating experience with statin drugs; the site also serves as a repository for information about statins, health conditions, and other people's personal experiences with statins.
Graveline took two courses of a statin medication for a total of five months. The first time he took the drug, in 1999, he lost his memory for six hours after which he stopped the drug. A year later, at the behest of his doctor, he tried it again. This second time he lost all memory beyond the age of 13 for twelve hours and never took a statin again. However, he was left with muscle damage from which he was never able to heal; he ultimately succumbed to statin-induced ALS in 2016. This is the beginning of his story:
When I first wrote of my personal side effects of Lipitor, my words were focused purely on transient global amnesia (TGA). This is because in 1999, shortly after this drug was started by my doctors at Johnson Space Center as part of my annual astronaut physical, this is what I experienced.
A year later, they re-started me on the same statin, Lipitor, at half the previous dose saying that my first 6-hour episode of TGA was only a coincidence.
Two months later I again experienced TGA. For twelve hours I was a thirteen-year-old high school student who knew my subjects, teachers and every kid in my class (according to my worried wife) but with no memory of my entire adult life.
I laughed when they told me I was married with children and a doctor. I could not have doctored a mouse and certainly had no children. I was thirteen! Fifty-six years of rich and fulfilled adult life had vanished from my mind as if it had never occurred. [Emphases added.]
The amnesia may have disappeared but Graveline found himself experiencing neuromuscular effects of the drug even though he had discontinued it.
After my recovery and after several years of research on statin drug side effects, I considered myself to be lucky to have had only TGA, for when it is over, you are back to normal. Not so for most of the other statin victims in my bulging repository with their persistent neuromuscular problems, short term memory loss and ALS and Parkinsonism-like reactions.
But now, having read thousands of reports from statin-damaged people, I wonder what the true effect of a statin really has been on my body? For suddenly, in two and one-half years, I have grown old.
By 2003 I had noted the gradual onset of unusual tiredness, easy fatigability and weakness. Cutting and splitting my own wood now required surprising effort. Then it seemed my low back and legs ached uncomfortably after only minimal exercise as if they had been strained excessively. I experienced no discomfort during sleep or recumbency, only after activity. My flowerbeds went untended. [Emphases added.]
Memory impairment not recognized as drug-related
Statin users experiencing cognitive impairment may not even link it to the cholesterol-lowering drugs they are taking. Such was the case with Jonathan McDonagh who had not thought to associate his memory problems with a drug for cardiac health until he forgot to refill his prescription and began feeling better, as was related by Michael Nedelmen for CNN Health:[15]
“I found myself slowly sinking into a sea of troubles,” McDonagh wrote in a medical journal in 2014, offering his perspective as a patient. “I didn’t connect my problems with the statin.”
Statins were also verified as causing neurocognitive disorder based on FAERS, the FDA adverse event reporting system, as research by Min Xiao, et al, published in the journal Expert Review of Clinical Pharmacology revealed.[16] Xiao, Min, et al. Expert Review of Clinical Pharmacology, vol. 17, no. 3, 31 Jan. 2024, pp. 255–261, doi:10.1080/17512433.2024.2311875.[/fn]
In the following tweet holistic practitioner Barbara O'Neill discusses the adverse effects of Lipitor and how one person recovered her memory after she stopped taking it:
In fact, as Law Dish author Samir explained, the initial class action suit against the FDA was filed by the Alzheimer's Association.[17]
Data on side-effects hidden from public scrutiny
In 2018, investigative medical reporter Dr. Maryanne Demasi brought to light the fact that the clinical trial data on the side effects of statins are not available for independent review. Instead, the data are being held by a group of researchers from Oxford University called the Cholesterol Treatment Trialists’ (CTT) Collaboration, led by Professor Sir Rory Collins. In a two-part report published on Michael West Media, entitled “Statin Wars: secrecy and the world’s most lucrative drugs,” Demasi writes,[18]
Who has them and where are the crucial data on the side-effects of statins?
The answer is it is held by the Cholesterol Treatment Trialists’ (CTT) Collaboration; the rather Orwellian title awarded to a group of researchers at Oxford University, led by Professor Sir Rory Collins.
While the CTT Collaboration periodically publishes its interpretation of the data on statins, what it does not do is permit independent researchers to verify CTT results by allowing access to the raw data.
I approached the CTT Collaboration in 2013 when doing research for the ABC’s TV program Catalyst. CTT researchers revealed that to gain access to the data from the drug companies, they would not be permitted to share the raw data with any third parties.
In a written statement, the CTT wrote:
“Such an agreement was necessary……without such an agreement the trial data could not have been brought together for systematic analysis”.
What does this mean? [Emphases added.]
The agreement, she says, undermines the purpose of science, which is meant to be questioned, not monopolized.
It means a legal instrument which had been drafted by drug companies effectively preserves their monopoly over the raw data of side-effects of statins.
This in itself is a matter for serious concern since science, by its very nature, requires contestibility. [Emphases added.]
Demasi explains that the legal agreement that was signed gave only one organization access to the raw data. Experts, doctors, and patients are thus forced to rely on that organization's interpretation of the data when making treatment decisions.
Further, while Professor Rory Collins has assured people that there are “few troubling side effects” associated with statin use even he publicly admits he has not seen the full data set on statin side effects.
The lack of independent scrutiny surrounding statin side-effects has ignited fresh concerns from some quarters within the medical profession.
The conclusions of the CTT Collaboration have influenced international guidelines for prescribing statins and have led to what has been called the ‘“Statinisation” of the population by Stanford University Professor, John Ioannidis. [Emphases added.]
Demasi quotes Professor Peter Gøtzsche of the Nordic Cochrane Collaboration who decried the secrecy and financial interests involved:
The whole issue is shrouded in secrecy and riddled with huge financial conflicts of interest, which does not instill public confidence. [Emphasis added.]
Turning healthy people into patients; let's not forget the children
Concealing clinical trial side effects data has made it virtually impossible for researchers and doctors to reach a uniform position regarding prescribing these medications. Demasi discussed this and more in her talk at a Cross-Fit Health event in June 2019. when she recounted her experience working for ABC (Australian Broadcasting Company). During her tenure there she “produced a two-part series called ‘Heart of the Matter,’ which challenged the role of cholesterol in heart disease and addressed the overprescription of statin drugs.” In her presentation, she accused drug companies and doctors of turning healthy people into patients:[19]
. . . so most of you know they [statins] are the most widely prescribed cholesterol-lowering medications in the world and an extremely lucrative drug class with Lipitor being the most profitable drug in the history of medicine.
There's been an exponential rise in the use of statins. We know that the early clinical trials showed that there was pretty good benefit for people at high risk of cardiovascular disease. So that's people who've already had a heart attack or a stroke and so they're in the secondary prevention category to prevent a second heart attack.
After recommending statins for those who might benefit, the “experts” began suggesting them for healthy people, and pediatricians considered screening children, as well, Demasi continued.
But then we started hearing from the experts and they were suggesting “Well, perhaps everybody over the age of 50 should be on these medications” even if you didn't have high cholesterol. So they were talking about medicating a rather healthy population of people and this is the primary prevention group of people that we're going to talk about and where the most debate lies.
Then we started hearing from pediatricians saying “well, perhaps we need to screen children for high cholesterol so we can screen for potential statin recipients,” and Pfizer even jumped on board and started marketing a grape-flavored statin in order to be more palatable for kids. (Emphases added.)
Demasi then explained the conflicting viewpoints on statin effectiveness — those who say that they've prevented “untold heart attacks and strokes” and those who say that they don't save lives, but may perhaps extend your life by less than a week.
So we have two sides — The proponents are saying statins are so safe and so effective they're prevented untold heart attacks and strokes, everybody should be on them.
Then we have the other side, who say “Well, no. They might protect a couple of people, but for the vast majority of people they don't really do much; they don't save lives because people still end up dying but they might prolong your life.” One study showed maybe three to four days.
So that's the two sides of the argument.
Time to recall Crestor?
Now, in 2024, Demasi is suggesting that Crestor be removed from the market. In a two-part series on her subscription substack, titled “Should Rosuvastatin (Crestor®) Be Withdrawn from the Market?” she reviews the drug's history and her basis for recommending its withdrawal. Part 1 is subtitled “The early safety warnings and how an aggressive marketing campaign helped catapult the drug's popularity”[20] and part 2 is subtitled “FDA's approval of rosuvastatin was largely based on a flawed trial prompting experts to call for the drug to be banned.”[21]
Check back for further installments of our series on cholesterol.
Updated Sept. 15, 2024 to identify Barbara O'Neill.
Footnotes:
[1] Arnett, Donna K, et al. “2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.” Circulation, U.S. National Library of Medicine, 10 Sept. 2019, www.ncbi.nlm.nih.gov/pmc/articles/PMC8351755/.
[2 ]In England, an additional 15 million people became eligible for statin treatment in the past year alone, after the country relaxed its prescribing guidelines for statins, the Guardian’s Andrew Gregory reported. Previously, only individuals with at least a 10% risk of developing heart disease within the next ten years could be prescribed a statin. Now, even those who fall in the mild risk category can take statin drugs if they want. (Gregory, Andrew. “New Statins Guidance Could Make Extra 15m People Eligible in England.” The Guardian, Guardian News and Media, 12 Jan. 2023, www.theguardian.com/society/2023/jan/12/new-statins-guidelines-nice-nhs-england.)
The National Institute for Health and Care Excellence says the scope for those who can be considered for the drugs should be widened dramatically – in what would be the single biggest change in a decade – to save thousands more lives.
. . .
Existing [official] guidance, covering about 10 million people in England, states that those with a 10% or higher risk over 10 years of a cardiovascular event, such as a heart attack or stroke, should be offered statins.
Now statins could also be considered as an option for people with even a small risk. The huge potential change comes after [the authorities] considered new evidence on the side-effects and safety of statins, meaning a wider group of people could be given them.
However, two years prior, the EMA (European Medicines Agency) limited statins to individuals with at least a 10% risk of developing heart disease within the next ten years. This was based on a 2013 study published in the BMJ that found the drug being overprescribed, after which the EMA conducted a comprehensive study and changed its recommendations to ensure the drugs would only be prescribed to people at high risk of heart disease.
Statins’ value as a primary defense against heart disease and stroke threats has been under intense scrutiny, particularly following the 2013 BMJ study results. Accusations revolving around overprescription and under-communication of the side effects, such as memory loss and muscle pain, sparked a fiery debate. Reservations from medical practitioners and patient groups increased, queering over the risk-benefit balance in low-risk heart disease individuals.
. . . the EMA conducted a comprehensive review of the evidence surrounding statins. Concluding its judgment in 2014, the EMA reasserted the safety and effectiveness of statins, particularly for patients with high cholesterol levels. However, the EMA only recommended statin prescriptions for high-risk heart disease individuals, a departure from prior lax prescription trends.
Controversy also exists surrounding the EMA’s revised guidelines. Medscape journalist Sue Hughes explains that some doctors take issue with the changes. (Hughes, Susan. “New European Guidelines ‘Drastically’ Reduce Statin Eligibility.” Medscape, 7 July 2022, www.medscape.com/viewarticle/976715?form=fpf.) The guidelines, according to the lead author, Dr. Martin Bødtker Mortensen of Denmark’s Aarhus University Hospital, are such that only 4% of the target population qualifies and they almost totally eliminate women. Low-risk countries do not qualify for statin use either.
“We have guidelines in place to try to prevent cardiovascular disease but the risk threshold in this new guideline means that almost nobody qualifies for treatment in many countries . . .
“We argue that the risk thresholds need to be lowered to get the statin eligibility in European countries to be in line with thresholds in the UK and US, which are based on randomized controlled trials,” he added.
[3] Moynihan, Ray, et al. “Selling Sickness: The Pharmaceutical Industry and Disease Mongering.” BMJ (Clinical Research Ed.), U.S. National Library of Medicine, 13 Apr. 2002, www.ncbi.nlm.nih.gov/pmc/articles/PMC1122833/.
[4] “Was a Double Mastectomy the Right Choice for Angelina Jolie?” What Doctors Don’t Tell You, 16 Oct. 2022, www.wddty.com/features/was-a-double-mastectomy-the-right-choice-for-angelina-jolie/
[5] “How Statin Drugs Protect the Heart.” Johns Hopkins Medicine, 3 Nov. 2021, www.hopkinsmedicine.org/health/wellness-and-prevention/how-statin-drugs-protect-the-heart#:~:text=Because%20many%20factors%20are%20involved,to%20be%20at%20high%20risk
[6] “High Cholesterol Facts.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, www.cdc.gov/cholesterol/facts.htm.
[7] “Statin Market: Global Industry Analysis and Forecast (2023-2029).” MAXIMIZE MARKET RESEARCH, 4 Oct. 2023, www.maximizemarketresearch.com/market-report/global-statin-market/77560/
[8] Antitrust lawsuits have also been filed. A $93 million settlement will allow Pfizer to move on from over twelve years’ worth of litigation due to antitrust lawsuits by drug distributors, Fierce Pharma reported. Companies filed suits against both Pfizer and Sun Pharma’s Ranbaxy Laboratories, claiming that Pfizer attempted to delay the sales of generic Lipitor through an illegal “reverse payment” agreement with Ranbaxy in which Pfizer gave the company its patents, permission to sell the drug in several countries, and six months exclusivity. (Becker, Zoey. “Pfizer Quells 12 Years of Lipitor Antitrust Litigation with $93m Settlement.” Fierce Pharma, 15 Feb. 2024, www.fiercepharma.com/pharma/pfizer-walks-away-over-decade-lipitor-antitrust-litigation-93m-settlement.) While Pfizer denies charges of wrongdoing, it has said that this settlement will allow the company to move on, as reported by Bloomberg Law: (Kaye, Danielle. “Pfizer Settles Lipitor Antitrust Lawsuit with $93 Million Payout.” Bloomberg Law, 16 Feb. 2024, www.news.bloomberglaw.com/antitrust/pfizer-settles-lipitor-antitrust-lawsuit-with-93-million-payout.)
Pfizer Inc. has agreed to pay $93 million to settle an antitrust lawsuit accusing the pharmaceutical giant of conspiring to delay sales of generic versions of the blockbuster cholesterol drug Lipitor.
The class settlement, announced in a motion filed Wednesday, is the culmination of more than a decade of multidistrict litigation brought by drug distributors in US District Court for the District of New Jersey. The distributors, including Burlington Drug Co. Inc. and Rochester Drug Co-Operative Inc., claimed Pfizer illegally paid pharmaceutical company Ranbaxy Laboratories to delay marketing generic versions of Lipitor and engaged in fraud when attempting to extend its Lipitor patent rights.
Despite agreeing to the settlement, a Pfizer spokesperson said the company denies wrongdoing, calling the allegations “factually and legally without merit.”
The settlement still needs a judge’s approval and lawsuits against Ranbaxy have yet to be settled.
Another antitrust lawsuit was settled for $70 million, which included lawyers’ fees of $23.3 million and $3.9 million in costs, by Merck & Co. Inc. and Glenmark Pharmaceuticals for colluding to delay the sale of a generic version of Merck’s cholesterol-lowering drug Zetia, as reported by Brendan Peirson for Reuters. In this case, several of the plaintiffs were municipal employee funds. (Pierson, Brendan. Merck, Glenmark Settle Antitrust Case over Cholesterol Drug For $70 mln, 19 Oct. 2023, www.reuters.com/legal/litigation/merck-glenmark-settle-antitrust-case-over-cholesterol-drug-70-mln-2023-10-19/.)
A group of drug wholesalers, who did not sue as a class, also reached a separate and confidential settlement at the same time.
[9]Weston. “Class Action Lawsuit against Statin Drugs.” Law Bench, 22 Aug. 2021, lawbench.org/class-action-lawsuit-against-statin-drugs/.
[10] Team USA Legal. “Lipitor Class Action Lawsuit - Do You Qualify?” USA Legal, 19 Nov. 2020, www.usalegal.com/lipitor-class-action-lawsuits/.
[11] Craine, Charles. “Lawsuits over Crestor, Lipitor, and Other Cholesterol Drugs (Statins).” Nolo, www.nolo.com/legal-encyclopedia/crestor-lipitor-other-cholesterol-drugs-29538.html.
[12] Ibid.
[13] Silvestrini, Elaine. “Crestor Lawsuits: Injuries, Misleading Ads and Settlements.” Drugwatch.Com, 5 Sept. 2023, www.drugwatch.com/crestor/lawsuits.
[14] Graveline, Duane, Dr. “My Statin Story.” Spacedoc.Com, www.spacedoc.com/articles/my-statin-story.
[15] Nedelman, Michael. “Statins: What Happens to Patients Who Stop Taking Them after Side Effects?” CNN, Cable News Network, 24 July 2017, www.edition.cnn.com/2017/07/24/health/statins-side-effects-outcomes-study/index.html.
[16] Xiao, Min, et al. Expert Review of Clinical Pharmacology, vol. 17, no. 3, 31 Jan. 2024, pp. 255–261, doi:10.1080/17512433.2024.2311875.
[17] Samir. “Class Action Lawsuits and the FDA’s Recall of Statins.” Law Dish, 19 July 2021,www.lawdish.com/class-action-lawsuits-and-the-fdas-recall-of-statins/.
[18] Demasi, Maryanne. “Statin Wars: Secrecy and the World’s Most Lucrative Drugs.” Michael West, 22 Jan. 2018, www.michaelwest.com.au/statin-wars-secrecy-and-the-worlds-most-lucrative-drugs/.
[19] “Dr. Maryanne Demasi: My Experience of Exposing the Statin Controversy.” YouTube, 13 Sept. 2019, www.youtube.com/watch?v=t2dHQSj90-A&t=284s.
[20] Demasi, Maryanne, Ph.D. “Part 1: Should Rosuvastatin (Crestor®) Be Withdrawn from the Market?”, Maryanne Demasi, reports, 29 Jan. 2024, www.blog.maryannedemasi.com/p/part-1-should-rosuvastatin-crestor.
[21] Demasi, Maryanne, PhD. “Part 2: Should Rosuvastatin (Crestor®) Be Withdrawn from the Market?” PART 2: Should Rosuvastatin (Crestor®) Be Withdrawn from the Market?, Maryanne Demasi, reports, 5 Feb. 2024, www.blog.maryannedemasi.com/p/part-2-should-rosuvastatin-crestor.


.webp)

